Tiny Clots
To treat or not to treat those little clots.
18 Mars 20163min

Sepsis Sofa
A new look at Sepsis criteria.
16 Mars 20162min

Priapism Management
A hard subject to discuss.
12 Mars 20164min

REBOA
Introduction of the use of REBOA for hemorrhagic shock.
11 Mars 20161min

Pediatric Procedures
Preparing for pediatric procedures in the ED.
11 Mars 20162min

Lemierre's Syndrome
An exploration of the presentation and diagnosis of Lemierre's Syndrome.
10 Mars 20163min

Sick Sinus Syndrome
An overview of Sick Sinus Syndrome.
9 Mars 20164min
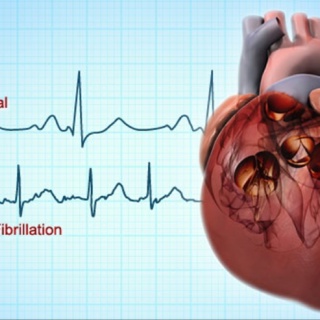
Medications for AFib
Comparison of medications used to treat atrial fibrillation.
8 Mars 20162min