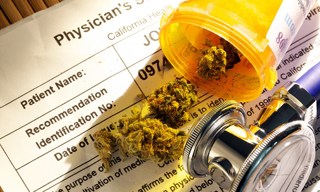
Brewcast Part IV: A Physician's Perspective on Medical Marijuana
Authors: Don Stader, M.D. & Peter Pryor, M.D. Topic: What caused Dr. Pryor to leave emergency medicine and enter the realm of medical marijuana?
5 Jul 201723min
Brewcast Part III: Cannabinoid Hyperemesis Syndrome
Author: Rachael Duncan, PharmD BCPS BCCCP Topic: Rachel explains the science behind one of the most common maladies thought to be induced by chronic cannabis use.
4 Jul 201714min

Brewcast Part II: Pharmacology of Cannabis
Author: Brett Marlin, M.D. Topics: Brett explains the biochemical and physiological properties of cannabis.
3 Jul 201718min
Brewcast Part I: The History of Cannabis in Medicine
Author: Don Stader, M.D Topic: Don kicks things off with an overview of the history of marijuana and how it has made its way into medicine.
2 Jul 201720min
Podcast #224: Troponin
Author: Sam Killian, M.D. Educational Pearls Not every troponin elevation is an MI. Trop elevates in about an hour in ACS and stays elevated for days. Non-MI conditions that cause elevated troponin: ...
1 Jul 20174min

Podcast #223: Acyclovir Toxicity
Author: Nick Hatch, M.D. Educational Pearls Acyclovir toxicity can uncommonly cause altered mental status, low blood glucose, hallucinations and myoclonic jerks. Toxicity often occurs in the setting ...
29 Jun 20172min

Podcast #222: Wells Criteria for PE
Author: Michael Hunt, M.D. Educational Pearls Wells Criteria was initially designed to screen patients for further workup for PE. Aspects of the Wells Criteria include: signs and symptoms of DVT (3...
27 Jun 20174min

Podcast #221: Walking Corpse Syndrome
Podcast #221: Walking Corpse Syndrome Author: Erik Verzemnieks, M.D. Educational Pearls Walking Corpse Syndrome (aka Cotard Delusion) is a very rare psychiatric disorder that leads to the belief that...
25 Jun 20171min