Podcast 694: Complete Heart Block
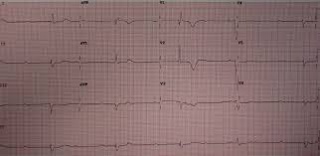
Contributor: Nick Hatch, MD Educational Pearls: Complete heart block or 3rd degree atrioventricular (AV) block is diagnosed via EKG and occurs when electrical signals from the sinoatrial (SA) node ar...
19 Jul 20214min

Podcast 693: Humerus Fractures
Contributor: Nick Tsipis, MD Educational Pearls: Humerus fractures can be characterized as proximal, midshaft, and distal fractures Proximal humerus fracture is the second-most common fracture in eld...
14 Jul 20217min

Podcast 692: Pelvic Fractures
Contributor: Peter Bakes, MD Educational Pearls: Pelvis is comprised of the iliac, ischium, and sacrum Three mechanisms for pelvic fractures by Young-Burgess Classification Anterior-posterior compr...
13 Jul 20214min

Podcast 691: TXA in Head Bleeds
Contributor: Ricky Dhaliwal, MD Educational Pearls: CRASH 3 Trial looked at over 12,000 patients with traumatic intracranial bleeds, randomizing patients to a therapy with TXA or standard of care wit...
12 Jul 20212min

Podcast 690: Rectal Oxygen. Nice,
Contributor: Chris Holmes, MD Educational Pearls: In the 1700s, boxes lined the River Thames to pump smoke up the rectum to resuscitate people who had been found unconscious in the river Sea cucumber...
7 Jul 20213min
Podcast 689: Peri-Intubation Hypotension
Contributor: Ricky Dhaliwal, MD Educational Pearls: Hypotension in patients requiring intubation should be resuscitated as much as possible While intubating, the negative inspiratory pressure goes aw...
6 Jul 20214min

Podcast 688: tPA Before Thrombectomy
Contributor: Aaron Lessen, MD Educational Pearls: DEVT Trial, a recent non-inferiority study, looked at giving tPA prior to endovascular thrombectomy and was stopped early because there was no benefi...
5 Jul 20212min
Podcast 687: STI Complications
Contributor: Jared Scott, MD Educational Pearls: PID (pelvic inflammatory disease) occurs when the infection ascends into the uterus Tubo-ovarian abscess occurs when the infection ascends to the fall...
30 Jun 20214min